
EM Quick Hits Video on Brugada Syndrome with Jesse McLaren
The 3 questions to diagnose Brugada Syndrome
Brugada syndrome is a sodium channelopathy that is temperature sensitive and causes an ECG pattern in the right ventricular leads (V1-V2) that is made worse with fever or sodium channel blockade. Brugada syndrome can lead to syncope or sudden cardiac death that can be prevented with an ICD. Making this diagnosis can save a life. To make the diagnosis, there are 3 questions that you must ask yourself.
Question #1: Does the ECG have a Brugada pattern?
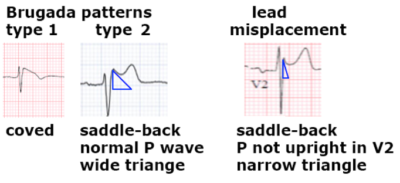
Type I: RS complex followed by a coved ST elevation that descends and ends into inverted and symmetric T wave. This is specific for Brugada pattern.
Type II: is RSR’ with saddleback ST elevation and positive T wave. This type can be seen with lead misplacement or normal variants.
- P waves are normally biphasic in V1 and fully upright in V2. If p wave is negative in V1 or not fully upright in V2 then the leads are too high which can produce an RSR’ pattern with ST elevation, this resolves with appropriate lead placement.
- If the P waves are as they should be, then draw a triangle with the peak at the R’ and base 5mm below. If the base is wide (> 4mm) this identifies Type II Brugada pattern. If the base is narrow, then this is a normal variant.
Question #2: If there is a Brugada pattern, is this a Brugada phenocopy/mimic?
Brugada phenocopies are reversible clinical conditions unrelated to fever or sodium channel blockade that can mimic Brugada pattern. This includes metabolic conditions that alter conduction (hyperkalemia, hypocalcemia, hypothyroidism, hypothermia), mechanical compression of the right ventricle (i.e., due to tension pneumothorax), V1-V3 ischemia (anterior infarct, PE), or myo/pericarditis. Once these conditions are treated the Brugada pattern should resolve.
Question #3: Does the patient have Brugada Syndrome?
If there is a confirmed Brugada pattern, and no evidence of a phenocopy the diagnosis of the syndrome requires that Type 2 converts to Type 1 with use of sodium channel blockers, or for the initial presence of type 1. Management of the syndrome depends on symptoms including syncope, nocturnal agonal breathing, or resuscitative arrest. Patients that have any of these require referral for ICD, whereas those incidentally found can be referred to electrophysiology. All patients should be instructed to treat fevers aggressively and avoid sodium channel blockers.
In summary, ask yourself these 3 questions:
-
- Is there a Brugada pattern or is this lead misplacement/normal variant?
- Are there any reversible causes that could lead to Brugada phenocopy?
- Does the patient have symptoms that fit diagnosis of the syndrome and need ICD, or do they just need a referral to electrophysiology?
Leave A Comment