
In this ECG Cases blog we look at how the multiple brush strokes of the ECG can be combined into an overall impression – to identify false positive STEMI, subtle Occlusion MI, and other emergencies…
Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. April 2025
Six patients presented with potentially ischemic symptoms. Can you use your impression from all the ECG brush strokes to identify which had occlusion MI, and which had other emergencies?
Case 1: 70 year old diabetic with epigastric pain and vomiting
–
Case 2: 55 year old with chest pain

–
Case 3: 20 year old with recurring shortness of breath on exertion

–
Case 4: 55 year old acute shortness of breath
–
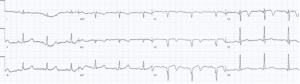
Case 5: 70 year old with chest pain and vomiting
–
Case 6: 60 year old with chest pain

–
The art of impression in occlusion MI
Let’s put the art in heart! This is the third in a series of blog posts looking at art of Occlusion MI: how we can use visual concepts to identify acute coronary occlusion, and how art helps explain the science of OMI. The first looked at mirror images, the second at scale and proportion, and this blog post looks at overall impression.
An impressionist painting is made up of multiple colours and distinct brush strokes, which come together to capture a moment in time. Similarly, an ECG captures a moment in time made up of multiple different and interacting parts of cardiac electrophysiology.
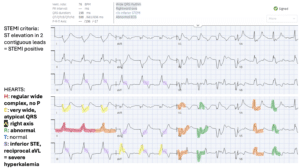
But STEMI criteria only looks at one feature – ST segment elevation – in isolation from all the rest. This would be like looking at Monet’s water lilies and only seeing the white paint, which could confuse us into thinking we are looking at clouds instead of the water that is reflecting them. On the other hand, computer interpretations can often identify multiple abnormalities, but fail to integrate them into an overall impression. This would be like seeing all of Monet’s separate brush strokes but failing to integrate them into an overall impression of water lillies on a pond.
Using the HEARTS approach for systematic ECG interpretation (Heart rate and rhythm, Electrical conduction, Axis, R-wave progression, Tall/small voltages and ST/T changes) looks at all the brush strokes of the ECG and integrates them into an overall impression. This can help identify false positive STEMI, subtle occlusion MI, and other emergencies.
For example, using multiple OMI findings (such as acute Q wave, subtle STE, reciprocal STD, hyperacute T waves, and reciprocal TWI), can double the sensitivity of STEMI criteria for acute coronary occlusion.[1] Similarly, PE and hyperkalemia can produce multiple ECG changes that on their own are non-specific, but combined and applied in clinical context can guide management.
Back to the cases
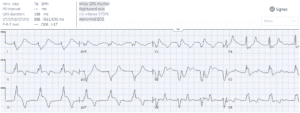
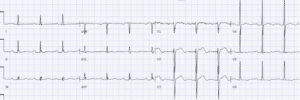
Case 1: 70 year old diabetic with epigastric pain and vomiting
Treated empirically with calcium. Potassium level 9.5 secondary to DKA and AKI. Follow up ECG normalized:
–
Case 2: 55 year old with chest pain
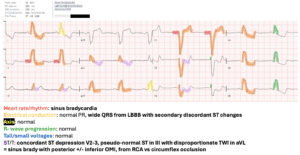
Missed OMI. ECG repeated 2 hours later after first trop returned at 2,000:

Ongoing posterior and now concordant STE in III with reciprocal change in aVL.
Cath lab activated: 100% RCA occlusion. Discharge ECG showed return of discordant ST change:
–
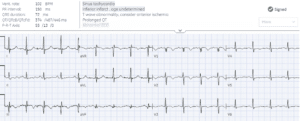
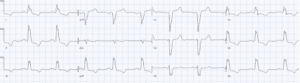
Case 3: 20 year old with recurring shortness of breath on exertion
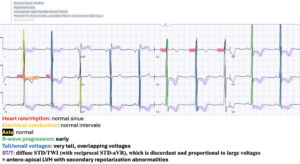
Troponins normal. Echo showed apical hypertrophic cardiomyopathy
–
Case 4: 55 year old acute shortness of breath
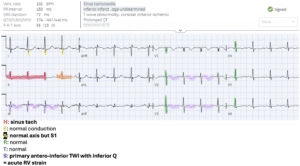
CT chest showed massive PE
–
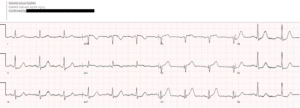
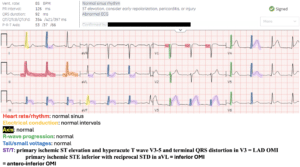
Case 5: 70 year old with chest pain and vomiting
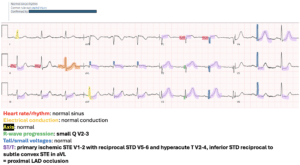
Cath lab activated: proximal LAD occlusion
Discharge ECG had full anterior R wave, and antero-lateral reperfusion TWI:
–
Case 6: 60 year old with chest pain
Patient had VF at triage after the ECG, was defibrillated and then cath lab activated: 100% mid LAD occlusion which cut off collateral circulation to a chronically occluded RCA, mimicking distal LAD occlusion. Follow up ECG had anterior reperfusion TWI:

–
Take home points for The Art of Occlusion MI Part 3 – Impression
- Use a systematic approach to interpret every ECG: Heart rate/rhythm, Electrical conduction, Axis, R-wave progression, Tall/small voltages, and ST/T changes
- Integrating multiple abnormalities can identify false positive STEMI, subtle Occlusion MI, hyperkalemia, and acute RV strain
For small group, live and highly interactive ECG courses, visit www.heartsECGcourse.com.
References for ECG Cases 55 – the Art of Occlusion MI, part 3: impression
- Meyers HP, Bracey A, Lee D, et al. Accuracy of OMI ECG findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. Int J Cardiol Heart Vasc 2021


Leave A Comment