cardiology emergency medicine
ECG Cases 39 – Transient STEMI Pitfalls and Pearls
In this ECG Cases blog we look at 9 patients with possible transient STEMI and discuss pitfalls and pearls in ECG interpretation and management...

cardiology emergency medicine
In this ECG Cases blog we look at 9 patients with possible transient STEMI and discuss pitfalls and pearls in ECG interpretation and management...
Dr. Jesse McLaren discusses some key aspects of cocaine chest pain ECG interpretation in this month's blog including: Patients with cocaine-associated chest pain require benzodiazepines +/- nitroglycerine for symptom relief, aspirin and ECG to look for signs of occlusion and reperfusion. In patients with chest pain + ST elevation, consider false positive STEMI including early repolarization, LVH and Brugada-pattern. In patients with cocaine chest pain who are STEMI negative, beware STEMI(-)OMI including subtle ST elevation, hyperacute T waves, reciprocal change, and refractory ischemia. For cocaine chest pain patients who's chest pain has resolved, look for reperfusion T wave inversion, as this may put them at risk for reocclusion.

In this EM Quick Hits podcast: Justin Morgenstern on fluids in pancreatitis, Leeor Sommer on nasal fractures, Christina Shenvi on delirium, Sheldon Cheskes and Rohit Mohindra on Dose VF, and Noor Khatib and Kari Sampsel on intimate partner violence...
While most of us have a clear algorithm in our minds for the management of life-threatening hyperkalemia, the same may not be said about the other life-threatening electrolyte abnormalities. In this ECG Cases blog Dr. Jesse MacLaren gives us an approach to potassium, calcium and magnesium abnormalities including risk factor assessment, ECG interpretation and management pearls...
On this month's EM Quick Hits podcast: Best of University of Toronto EM with Yaron Finkelstein on pediatric cannabis poisoning pitfalls, Brit Long on recognition and management of esophageal perforation, Jesse McLaren on 3 questions to diagnose Brugada Syndrome, Tahara Bhate on QI Corner, Constance Leblanc on maintaining wellness in career transitions from CAEP 2022...
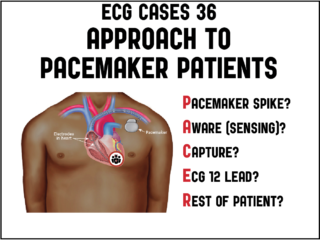
In this month's ECG Cases blog Dr. McLaren explains the PACER mnemonic approach to patients with pacemakers: Pacemaker spike: is it appropriately presence/absent, is there pacemaker-mediated tachycardia (apply magnet) or is there failure to pace (apply magnet to stop sensing, cardio consult)? Aware (sensing): is it normal, is there oversensing (underpacing: apply magnet) or undersensing (treat reversible causes, cardio consult). Capture: if there are pacemaker spikes is there capture, or failure to capture (treat reversible causes, cardio consult). ECG 12 lead: are there signs of hyperkalemia (extra wide QRS, peaked T) or Occlusion MI (Modified Sgarbossa Criteria) that need immediate treatment. Rest of patient: is there a complication of pacemaker insertion related to the pocket (hematoma, infection), lead (pneumothorax, DVT), or heart (pericardial perforation), or is there an emergency unrelated to the pacemaker (eg dehydration, sepsis, GI bleed)...

Takotsubo Syndrome is usually triggered by an emotional or physical stress leading to acute catecholaminergic myocardial stunning. The initial ST elevation phase of Takotsubo Syndrome mimics Occlusion MI, can not be distinguished by patient factors or POCUS findings, and requires immediate angiogram. The subsequent phase of Takotsubo Syndrome has T wave inversion in an apical distribution, which can mimic reperfusion, but often has very deep T wave inversions and a very long QT interval. Takotsubo Syndrome is a retrospective diagnosis of exclusion—with an angiogram ruling out occlusion, a ventriculogram showing apical ballooning, and a follow up echo showing recovery of LV function. Complications of Takotsubo Syndrome include LV failure, apical thrombus, and polymorphic VT from long QT. Jesse McLaren guides us through 10 ECGs to elucidate these important take home points...
Which patients with ECG evidence of coronary occlusion require a CT scan to rule out aortic dissection? What are the range of ECG findings in acute aortic dissection and how do they change management? Dr. Jesse McLaren guides us through 9 cases to answer these and other questions on ECG interpretation in aortic dissection...
In this main episode podcast, Dr. David Carr joins Anton to give us his simplified approach to syncope based solely on history, physical and ECG to help guide disposition decisions. We answer questions such as: What features have the best likelihood ratios to help distinguish syncope from seizure? What key clinical features on history and physical exam can help us distinguish orthostatic and reflex syncope from the more sinister cardiac syncope? What is the best approach to ECG interpretation for the patient who has presents with syncope? Are syncope clinical decision tools any better than physician gestalt? and many more.... Please support EM Cases by giving a donation: https://stg-emergencymedicinecases-emcstaging.kinsta.cloud/donation/
In this month's EM Quick Hits podcast: Anand Swaminathan on GI balloon tamponade preparation and indications, Jesse McLaren on why troponin is rarely useful in SVT, Christina Shenvi on why we should not use the term "mechanical fall" in older patients, Nour Khatib & Jonathan Wallace on rural vertical vertigo case and Reuben Strayer on VAFEI - Video-Assisted Flexible Endoscopic Intubation for the anatomically challenging airway...